
 When it comes to physical anthropology and skull shapes race is a highly contentious issue. It’s not clear-cut because there are many variations among races. To keep it simple I refer to the different skull shapes as square, rectangular and round designs based on their overall outlines and the shapes of the orbits of the eyes and nose.
When it comes to physical anthropology and skull shapes race is a highly contentious issue. It’s not clear-cut because there are many variations among races. To keep it simple I refer to the different skull shapes as square, rectangular and round designs based on their overall outlines and the shapes of the orbits of the eyes and nose.
Basically there are three distinct shapes in the design of the human skull, European, Asian and African. Although, there are slight variations, the cranial capacity is roughly the same and varies from about 1200 to 1800 cc. Asians tend to have the largest cranial capacity followed in size by European and African designs. Regardless of size, however, humans have roughly the same amount of nerves in the brain. Larger brains simply have larger nerves and support tissues, not necessarily more nerves.
The human brain is relatively large compared to body size. The base of the skull, however, is relatively short. This short base is due to forward migration of the foramen magnum over time toward the middle of the skull beneath the mass of the head and brain. The foramen magnum is the large hole in the base of the skull through which the brainstem passes to the cord.
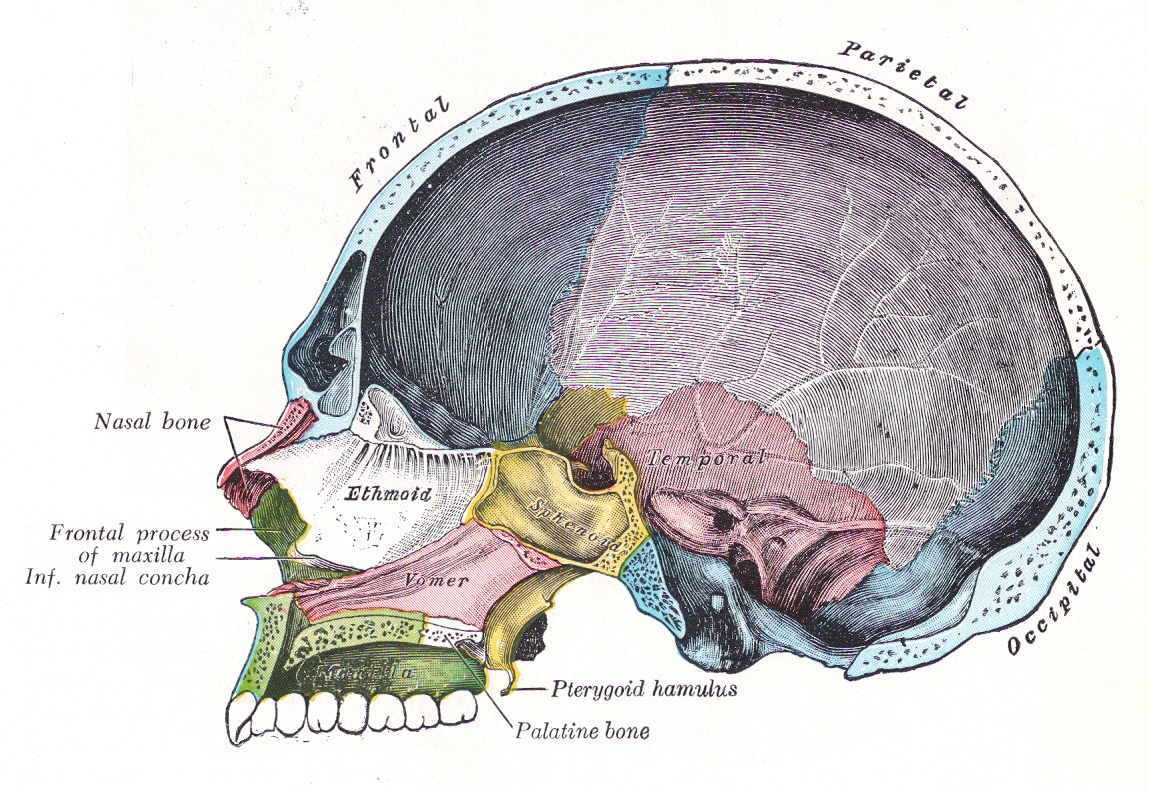
 In the picture on the left the front part of the base of the skull is from the back of the nose to the notch in the yellow colored bone called the sella turcica where the pituitary gland is located. Unlike the picture, it tends to slop upwards slightly. The base then bends downward at a steep angle along the back of the yellow colored bone and along the blue colored bone. Technically, together the two bones are called the clivus portion of the base. The face of the brainstem and most of the cranial nerves are located just above the clivus. The foramen magnum for the cord is at the bottom of the clivus. The rear portion of the base extends behind the foramen magnum. The rear portion of the base is also called the posterior fossa. The base of the posterior fossa also slopes upwards.
In the picture on the left the front part of the base of the skull is from the back of the nose to the notch in the yellow colored bone called the sella turcica where the pituitary gland is located. Unlike the picture, it tends to slop upwards slightly. The base then bends downward at a steep angle along the back of the yellow colored bone and along the blue colored bone. Technically, together the two bones are called the clivus portion of the base. The face of the brainstem and most of the cranial nerves are located just above the clivus. The foramen magnum for the cord is at the bottom of the clivus. The rear portion of the base extends behind the foramen magnum. The rear portion of the base is also called the posterior fossa. The base of the posterior fossa also slopes upwards.
 In some skulls the angle of the clivus is relatively steep. In others it is flatter. Regardless of the angle of the clivus, all humans are predisposed to the brainstem sinking into the foramen magnum due to its location beneath the skull. A Chiari malformation occurs when the brainstem sinks into the foramen magnum as seen in the brain scan to the right.
In some skulls the angle of the clivus is relatively steep. In others it is flatter. Regardless of the angle of the clivus, all humans are predisposed to the brainstem sinking into the foramen magnum due to its location beneath the skull. A Chiari malformation occurs when the brainstem sinks into the foramen magnum as seen in the brain scan to the right.
Typically, the brainstem is surrounded by cisterns filled with cerebrospinal fluid (CSF) which allows the brain to float above the foramen magnum and base of the skull thus preventing contact with the bones of the base and foramen magnum. In a Chiari malformation, it is typically the tonsillar portion of the cerebellum that gets trapped in the foramen magnum.
In this regard, among other things, the design of the posterior fossa may explain why people of European race have a much higher incidence of multiple sclerosis than people of Asian and African races. While the floor of the posterior fossa slopes slightly upwards in all races, it is considerably shorter in European skulls than it is in Asian and African ones. The rear wall of the posterior fossa in European skulls also slant outward. Thus European designs tend to crowd the cerebellum, comparatively speaking, from front to back more than Asian and African designs. They also pitch the cerebellum forward and downward toward the foramen magnum. Additionally, the design of the shorter sloped floor and slanted rear wall also affects the length, pitch and layout of the drainage system of the brain. Shorter distances and reduced angles in the base of the European skull most likely reduces curves and provides less resistance to reverse flows of venous blood in the dural sinuses.
Lastly, in contrast to European skulls, the jaws of Asian skulls are more in line with the face which improves balance on top of the cervical spine and makes them more energy-efficient. Protruding muzzles in European designs also create greater swing weights when the head is whiplashed as in trauma. In contrast to taller and narrower European and Asian skull faces, African skulls have shorter, wider and deeper faces. The lower wider face lowers the center of gravity and swing weight, and like Asian skulls, may provide better protection to the head and neck, as well as the brain and cord in whiplash type traumas.
In brief, the similar designs of the Asian and African posterior fossa of the rear portion of the base of the skull may provide better protection for the brain from whiplash, inversion flows and classic MS. On the other hand, it may also explain why Asian and African races tend to get a variant of MS called optic-spinal multiple sclerosis and Devic’s disease. Both conditions are associated with optic neuritis and transverse myelitis rather than classic MS lesions, signs and symptoms.
The different signs and symptoms in the above conditions may be the consequence of different points of contact and compression of the underside of the brain against the base of the vault and within the foramen magnum. The differences in contact points may be due to design differences in the base of the skull. In my next post I will discuss the location of the brainstem and cranial nerves in relationship to the base of the skull and foramen magnum. Their location makes them highly susceptible to compression by either an increase or a decrease in CSF volume in the cisterns.
For additional information on this and related topics visit my website at http://www.upright-health.com.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Another brilliant post, Dr. Flanagan!
Differences in our skulls, based on our race, are impossible to ignore. I extrapolate some of your thoughts to similar differences in skeletal variations within families (I am from a family of small heads and short posterior fossas, for example) and other skeletal anomalies that may not be readily apparent (a Marfan phenotype, for instance).
I believe that what you are describing is going to open the door for an incredible number of patients who have had illnesses and disabilities that no one has yet been able to quite put their finger on…
I eagerly await your next post, as the CSF volume in the cisterns will likely answer numerous questions for doctors and patients alike.
Thank you, again, for generously sharing your thoughts and advise.