
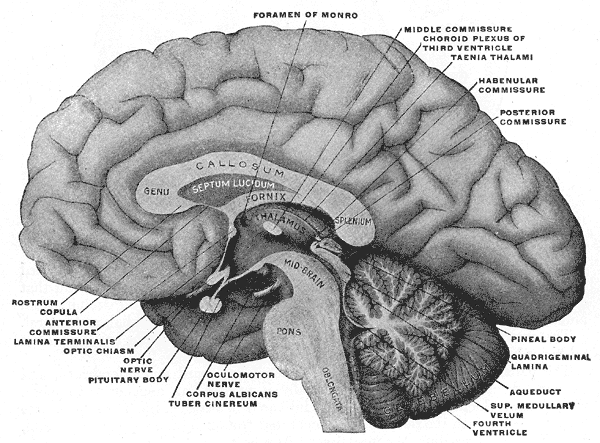
 The midbrain is the smallest structure in the brain and is positioned on top of the brainstem. In the picture to the right, it can be seen located between the thalamus and hypothalamus of the diencephalon above, and the pons and medulla of the lower brainstem below. The thalamus located on top of the midbrain, forms the walls of the third ventricle. Among other things, atrophy of the thalamus and enlargement of the third ventricle (ventriculomegaly) have been associated with multiple sclerosis (MS).
The midbrain is the smallest structure in the brain and is positioned on top of the brainstem. In the picture to the right, it can be seen located between the thalamus and hypothalamus of the diencephalon above, and the pons and medulla of the lower brainstem below. The thalamus located on top of the midbrain, forms the walls of the third ventricle. Among other things, atrophy of the thalamus and enlargement of the third ventricle (ventriculomegaly) have been associated with multiple sclerosis (MS).
In contrast to the ventricles, which are in the core of the brain, the cisterns surround the midbrain. Enlargement of either can be a sign of atrophy. Enlargement of the cisterns along with atrophy of the midbrain has been associated with variations of Parkinson’s called progressive supranuclear palsy, vascular Parkinson’s, vascular dementia, multisystem atrophy, and an Alzheimer’s variation called Lewy-body dementia.
Some of the characteristics of vascular Parkinson’s and vascular dementia overlap. Both conditions are associated with a more frequent occurrence of brain atrophy, white matter lesions and a predominance of motor symptoms, such as gait disturbances. Several clinical features of vascular Parkinson’s, including early postural instability, pseudobulbar phenomena, and predominance of lower body signs, further suggest that vascular Parkinson’s may be associated with atrophy of the brainstem.
In addition to the neurodegenerative conditons above, atrophy of the midbrain has also been associated with MS. More often, however, MS is associated with enlargement of the cerebral aqueduct of the ventricular system, especially the upper portion located adjacent to the third ventricle, mentioned above. In any case, researchers now suspect that the midbrain is particularly sensitive to neurodegenerative conditions. They offer no explanation, however, as to why it is particularly sensitive. One possible explanation, may be because of its exposure to cerebrospinal fluid (CSF) hydraulics in the ventricular system and cisterns.
The midbrain is surrounded by cisterns filled with CSF. CSF also passes from the third ventricle through the cerebral aqueduct in the midbrain to the fourth ventricle below. The portion of the midbrain located behind the aqueduct is called the tectum. The portion in front is called the tegmentum. The midbrain is associated with sight, sound, motor control, the sleep-wake cycle, alertness and temperature regulation. It also contains pathways for communication and coordination between the higher and lower centers of the brain, brainstem and spinal cord including the long motor tracts that descend to the cord to supply the muscles and the sensory nerves that deliver information from receptors in the body to appropriate centers in the brain.
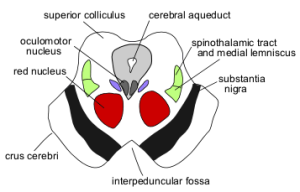 As shown in the sketch of the midbrain on the left, the cerebral aqueduct is surrounded by gray unmyelinated nerves called the periaqueductal gray matter, which contains the reticular formation of the brainstem. The reticular formation contains functional cell groups that are important for control of eye, head, or lid movements. The mesencephalic reticular formation is primarily involved in the control of vertical gaze. Vertical gaze is sometimes affected in Parkinson’s disease and MS. The dark gray band on the ventral (front) side of the midbrain is the substantia nigra which produces a neurotransmitter called dopamine. Atrophy of the substantia nigra and decreased dopamine production are hallmark signs of primary Parkinson’s disease. Among other things, decreased dopamine production causes resting tremors in Parkinson’s.
As shown in the sketch of the midbrain on the left, the cerebral aqueduct is surrounded by gray unmyelinated nerves called the periaqueductal gray matter, which contains the reticular formation of the brainstem. The reticular formation contains functional cell groups that are important for control of eye, head, or lid movements. The mesencephalic reticular formation is primarily involved in the control of vertical gaze. Vertical gaze is sometimes affected in Parkinson’s disease and MS. The dark gray band on the ventral (front) side of the midbrain is the substantia nigra which produces a neurotransmitter called dopamine. Atrophy of the substantia nigra and decreased dopamine production are hallmark signs of primary Parkinson’s disease. Among other things, decreased dopamine production causes resting tremors in Parkinson’s.
There are many different types of midbrain syndromes. Two well known midbrain syndromes, called Parinaud’s syndrome and dorsal midbrain syndromes, have been associated with Parkinson’s disease, dementia and MS. Dorsal midbrain syndromes are associated with difficulty looking up, diplopia, blurred vision, oscillopsia (symmetrical eye tremors), as well as other accompanying neurological symptoms. It is sporadic. The causes are obstructive hydrocephalus, hemorrhages in the midbrain, MS, AV malformations, trauma, and compression, such as from pineal tumors.
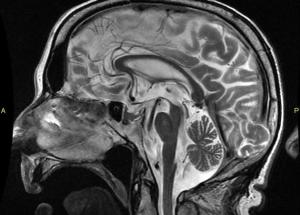 Atrophy of the midbrain is most commonly associated with progressive supranuclear palsy, mentioned above. The atrophy causes a characteristic deformation of the midbrain that radiologists refer to as the hummingbird sign when viewed from the sagittal view (side) because it looks like a small bird with a large beak, as seen in the brain scan on the left. The brain scans on the left and below are used with permission from a collection by Dr. Frank Gaillard of Radiopaedia.com. The hummingbird shape is seen at the top portion of the long, dark gray structure (brain stem) in the middle of the brain. There is a long, thin, curved beak-like projection in front and a big round structure below, which is the pons portion of the brainstem. The hummingbird sign is also called the penguin sign. In either case, the beak is the most telling feature of atrophy of the midbrain. The beak is part of the tectum on the dorsal (rear) surface of the midbrain. The tectum contains important nerve centers related to the control of eye muscles and sight. It also contains nerve centers related to sound.
Atrophy of the midbrain is most commonly associated with progressive supranuclear palsy, mentioned above. The atrophy causes a characteristic deformation of the midbrain that radiologists refer to as the hummingbird sign when viewed from the sagittal view (side) because it looks like a small bird with a large beak, as seen in the brain scan on the left. The brain scans on the left and below are used with permission from a collection by Dr. Frank Gaillard of Radiopaedia.com. The hummingbird shape is seen at the top portion of the long, dark gray structure (brain stem) in the middle of the brain. There is a long, thin, curved beak-like projection in front and a big round structure below, which is the pons portion of the brainstem. The hummingbird sign is also called the penguin sign. In either case, the beak is the most telling feature of atrophy of the midbrain. The beak is part of the tectum on the dorsal (rear) surface of the midbrain. The tectum contains important nerve centers related to the control of eye muscles and sight. It also contains nerve centers related to sound.
When viewed from top to 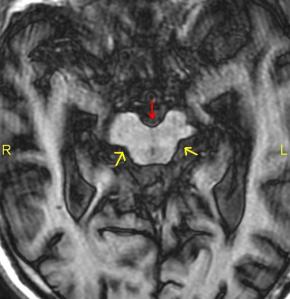 bottom looking down on the brain, which is called an axial view, the midbrain appears compressed front to back in a characteristic deformation. Radiologists call it the Mickey Mouse sign because it looks like a small round face with a little black nose and big round ears located in the center of the MRI on the right.
bottom looking down on the brain, which is called an axial view, the midbrain appears compressed front to back in a characteristic deformation. Radiologists call it the Mickey Mouse sign because it looks like a small round face with a little black nose and big round ears located in the center of the MRI on the right.
Progressive supranuclear palsy, also known as Steele-Richardson-Olszewski syndrome, is a rare disease. It gradually destroys nerve cells in parts of the brain that control eye movements, breathing, and muscle coordination. The loss of nerve cells causes palsy, or paralysis, that slowly gets worse as the disease progresses. The palsy affects the ability to move the eyes, relax the muscles, and control balance. The initial symptoms in two-thirds of the cases are loss of balance, lunging forward when mobilizing, fast walking, bumping into objects or people, and falls. Other common early symptoms are changes in personality, general slowing of movement, and visual symptoms.
Signs of progressive supranuclear palsy include: supranuclear ophthalmoplegia, rigid neck spasms called dystonia, Parkinsonism signs and symptoms, pseudobulbar palsy (difficulty swallowing and speaking), behavioral and cognitive impairment, imbalance and difficulties walking, as well as frequent falls. Atrophy of the midbrain appears to be more characteristic of vascular Parkinson’s and progressive supranuclar palsy than primary Parkinson’s which is typically associated with specific degeneration and atrophy of the substantia nigra. It’s also less severe in vascular Parkinson’s compared to progressive supranuclear palsy.
The cause of atrophy of the midbrain in Alzheimer’s and Parkinson’s disease, as well as enlargement of the cerebral aqueduct of Slyvius in MS is unknown. In addition to the aqueduct, MS is also associated with enlargement of the third ventricle that adjoins and drains into it. Ventriculomegaly and an enlarged cerebral aqueduct are signs of hydrocephalus. In contrast to the ventricles and cerebral aqueduct, enlarged cisterns are not necessarily a sign of hydroceplalus if not accompanied by enlargement of the ventricles. On the other hand, hydrocephalus is caused by obstruction to CSF flow that results in an increase in volume. One of the most likely places for blockage of CSF flow to occur is in the foramen magnum and upper cervical spinal canal. Blockage of CSF flow between the cranial vault and spinal canal can cause an increase in volume in the cisterns and subsequent compression of structures they surround such as the midbrain. Decreased blood flow and chronic ischemia may also play a role in atrophy of the midbrain but that’s another topic that will be discussed in future posts. In any case, malformations, misalignments and chronic deformation of the upper cervical spine may affect blood and CSF flow in the brain leading to chronic ischemia, edema and normal pressure hydrocephalus resulting in neurodegenerative conditions and diseases.
For further information on the role of the midbrain in neurodegenerative conditions, visit my website at www.upright-health.com. The cause behind many of the conditions above is discussed in my book, “The Downside of Upright Posture”. Information, of which, can also be found at the website.
 The brain scan on the right is of an adult patient with NPH. NPH is typically associated with ventriculomegaly without atrophy (shrinkage) of the brain. Atrophy is seen as a widening of the spaces of the brain called fissures and sulci (dark spaces between the folds in the picture) that separate the gyri and folds of the different lobes. Ventriculomegaly is usually found around the frontal and temporal horns of the
The brain scan on the right is of an adult patient with NPH. NPH is typically associated with ventriculomegaly without atrophy (shrinkage) of the brain. Atrophy is seen as a widening of the spaces of the brain called fissures and sulci (dark spaces between the folds in the picture) that separate the gyri and folds of the different lobes. Ventriculomegaly is usually found around the frontal and temporal horns of the  CSF from the fourth ventricle drains into the pontine cistern, the cisterna magna and the central canal of the
CSF from the fourth ventricle drains into the pontine cistern, the cisterna magna and the central canal of the  The brain scan on the right is of a child with a condition called Dandy-Walker Syndrome, which looks somewhat similar to the multisystem atrophy scan above. Here the fourth ventricle (the dark space in front of the cerebellum) and the prepontine cistern (the dark space in front of the cord) aren’t enlarged as above. Only the cisterna magna below the cerebellum is enlarged, which is called mega cisterna magna. Some cases of Dandy-Walker syndrome have enlarged ventricles, hydrocephalus and a mega cisterna magna. According to the classic definition, a mega cisterna magna alone, without ventriculomegaly, isn’t classified as hydrocephalus.
The brain scan on the right is of a child with a condition called Dandy-Walker Syndrome, which looks somewhat similar to the multisystem atrophy scan above. Here the fourth ventricle (the dark space in front of the cerebellum) and the prepontine cistern (the dark space in front of the cord) aren’t enlarged as above. Only the cisterna magna below the cerebellum is enlarged, which is called mega cisterna magna. Some cases of Dandy-Walker syndrome have enlarged ventricles, hydrocephalus and a mega cisterna magna. According to the classic definition, a mega cisterna magna alone, without ventriculomegaly, isn’t classified as hydrocephalus.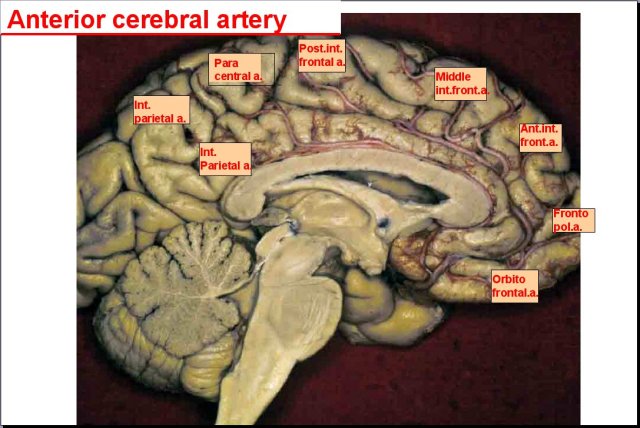
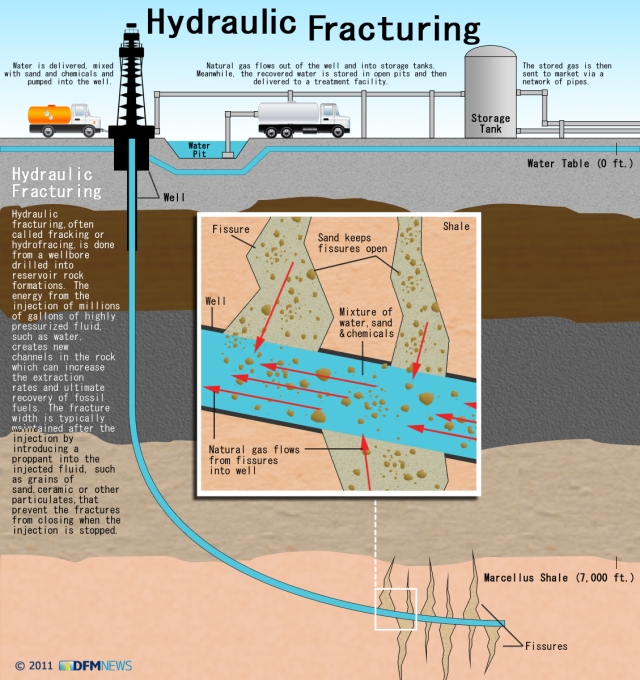
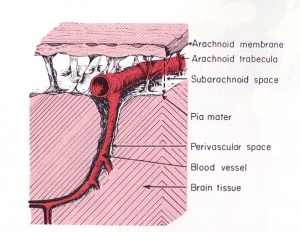 In contrast to hydrofracking which pumps large volumes of water into deep subterranean rocks, the heart pumps a relatively large volume of blood into the arteries contained within the subarachnoid space (see picture to the right). The subarachnoid space surrounds the outer surfaces of the lobes, the convolutions (gyri) and fissures of the brain and the brainstem within the cranial vault. The large incoming arteries pass through the subarachnoid space to supply numerous smaller branches (arterioles) that exit the subarachnoid space and enter tunnels called perivascular or Verchow-Robin spaces to supply smaller branches that supply the parenchyma (substance) of the brain.
In contrast to hydrofracking which pumps large volumes of water into deep subterranean rocks, the heart pumps a relatively large volume of blood into the arteries contained within the subarachnoid space (see picture to the right). The subarachnoid space surrounds the outer surfaces of the lobes, the convolutions (gyri) and fissures of the brain and the brainstem within the cranial vault. The large incoming arteries pass through the subarachnoid space to supply numerous smaller branches (arterioles) that exit the subarachnoid space and enter tunnels called perivascular or Verchow-Robin spaces to supply smaller branches that supply the parenchyma (substance) of the brain. Blockage of venous blood and cerebrospinal fluid anywhere along their pathways can alter CSF flow and cause abnormal pressure waves. The abnormal pressure waves are the result of incoming arterial blood flow and pressure waves running into resistance from venous backpressure and reduced or blocked CSF outflow causing what plumbers refer to as a water hammer. As shown in the sketch on the left, water hammers occur in domestic plumbing when water flow out of a faucet is suddenly shut off. This causes waves to be reflected backwards and crash with incoming waves. Since stiff non-elastic pipes can’t absorb the force like elastic veins, it causes them to shudder like a tremor. The tremor causes the pipes to bounce on surrounding structures resulting in noises that sound like someone hammering on the pipes.
Blockage of venous blood and cerebrospinal fluid anywhere along their pathways can alter CSF flow and cause abnormal pressure waves. The abnormal pressure waves are the result of incoming arterial blood flow and pressure waves running into resistance from venous backpressure and reduced or blocked CSF outflow causing what plumbers refer to as a water hammer. As shown in the sketch on the left, water hammers occur in domestic plumbing when water flow out of a faucet is suddenly shut off. This causes waves to be reflected backwards and crash with incoming waves. Since stiff non-elastic pipes can’t absorb the force like elastic veins, it causes them to shudder like a tremor. The tremor causes the pipes to bounce on surrounding structures resulting in noises that sound like someone hammering on the pipes. Dr. Hakim later called the condition he discovered
Dr. Hakim later called the condition he discovered  The dark gray spaces in front of the brainstem and beneath the cerebellum are called cisterns. CSF flows out of the fourth ventricle and into the cisterns. The cisterns cushion the brain from the hard walls of the cranial vault. They also support the brain and prevent it from sinking into the large hole in the bottom of the vault called the
The dark gray spaces in front of the brainstem and beneath the cerebellum are called cisterns. CSF flows out of the fourth ventricle and into the cisterns. The cisterns cushion the brain from the hard walls of the cranial vault. They also support the brain and prevent it from sinking into the large hole in the bottom of the vault called the  The term poroelasticity refers to the pores in soils and rocks that affect their elasticity. Elasticity is the ability of a structure to deform and return to its original shape without breaking (fracturing). The pores in soils and rocks can be filled with gas or fluids. The gas could be air or natural gas. The fluid could be water or oil. The gases or fluids affect the strength of soils and rocks, as well as their elasticity. Consequently, the gases and fluids affect the ability of soils and rocks to deform and reform. Structures that go through expansion and contraction are considered to be biphasic. If it can’t deform and reform, meaning return to its original shape, the structure is considered to be monophasic. The ability of a structure to deform and return to its original shape is determined by, what is called, its elastic coefficient.
The term poroelasticity refers to the pores in soils and rocks that affect their elasticity. Elasticity is the ability of a structure to deform and return to its original shape without breaking (fracturing). The pores in soils and rocks can be filled with gas or fluids. The gas could be air or natural gas. The fluid could be water or oil. The gases or fluids affect the strength of soils and rocks, as well as their elasticity. Consequently, the gases and fluids affect the ability of soils and rocks to deform and reform. Structures that go through expansion and contraction are considered to be biphasic. If it can’t deform and reform, meaning return to its original shape, the structure is considered to be monophasic. The ability of a structure to deform and return to its original shape is determined by, what is called, its elastic coefficient.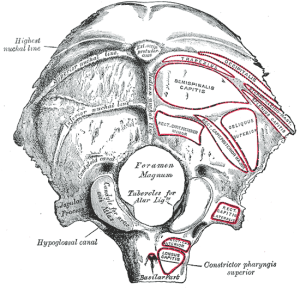 While it is not considered to be a factor that directly affects compliance (elasticity) in the brain, the foramen magnum and spinal canal play an important role in maintaining CSF volume and pressure in the brain. As shown in the picture on the left of the skull base, the foramen magum is the large hole in the base of the skull that connects the cranial vault to the spinal canal. The arterial pulsations and pressure waves that are pumped into the brain by the heart are not only buffered but a proportionate outflow in the amount of blood and CSF is also transferred out of the cranial vault and brain through the foramen magnum and into the spinal canal.
While it is not considered to be a factor that directly affects compliance (elasticity) in the brain, the foramen magnum and spinal canal play an important role in maintaining CSF volume and pressure in the brain. As shown in the picture on the left of the skull base, the foramen magum is the large hole in the base of the skull that connects the cranial vault to the spinal canal. The arterial pulsations and pressure waves that are pumped into the brain by the heart are not only buffered but a proportionate outflow in the amount of blood and CSF is also transferred out of the cranial vault and brain through the foramen magnum and into the spinal canal.















{kind=link}
{kind=link}
{kind=link}